




Abstract
Objectives:
To assess body composition and bone changes pre- to post-season (pre-post) and post- to off-season (post-off) in female soccer athletes (SC).
Methods:
Outcomes were assessed using DXA and pQCT in 23 SC and 17 controls at three times throughout season.
Results:
SC, non-starters in particular, lost lean mass pre-post (-0.9±0.2 kg, p<0.01; not different from controls, p=0.2) and gained fat mass post-off (1.4±0.3 kg, p<0.01; differed from controls, p=0.01). Baseline femoral neck and hip aBMD were higher in SC than controls (both, p<0.04), but increased in controls more than SC in pre-post and decreased post-off. SC cortical bone mineral content (BMC), cortical area and periosteal circumference increased pre-post (all, p<0.01; differed from controls, p<0.05) and trabecular vBMD decreased post-off (-3.0±1.3 mg/cm3; p=0.02; not different from controls, p=0.4). Both SC and controls increased cortical BMC, cortical area, and thickness post-off (all, p<0.01).
Conclusion:
Soccer players lost lean mass over the competitive season that was not recovered during off-season. Bone size increased pre- to post-season. Female soccer athletes experience body composition and bone geometry changes that differ depending on the time of season and on athlete’s playing status. Evaluations of athletes at key times across the training season are necessary to understand changes that occur.
Keywords: Bone, Athletes, Female, pQCT, DXA
Introduction
Collegiate soccer athletes spend multiple hours per week meeting the physical demands of their sport. This includes time spent conditioning, strength training, practicing and competing in games throughout the season as well as continued conditioning and training throughout the off-season. Participation in collegiate athletics is known to influence multiple physiological parameters including but not limited to body composition, muscle strength, and bone characteristics[1,2]. However, few studies have examined potential changes in these parameters over the competitive soccer season and into the off-season in female athletes[3-5].
Body composition may differ by sport due to sport-specific training and performance expectations[3]. During the off-season (end of a competitive season until the next competitive season), soccer players generally participate in a periodized strength and conditioning program designed to optimize agility, speed, aerobic and anaerobic capacities. During the competitive in-season period (typically August through November), strength and conditioning training is replaced with team training, competitions, injury rehabilitation and recovery. Some studies involving soccer athletes have reported decreases in lean mass from pre-season to post-season[3,4] while others have reported no change or gains in lean mass over the competitive season[5-7]. However, these studies used different methods (hydrostatic weighing or dual-energy x-ray absorptiometry, DXA) to measure body composition and performed these measures at different times of the season which may explain inconsistencies among results.
Many studies assessing the effect of sport participation on bone density are cross-sectional and provide data from one time point during a competitive year. Cross-sectional studies indicate a positive effect of collegiate sports participation on areal bone mineral density (aBMD) for total body and at regional sites in female athletes compared to non-active controls[1,2,8-13]. Additionally, odd-impact loading sports such as soccer and tennis appear to have a similar osteogenic effect on bone compared to high-impact loading sports such as volleyball and hurdling due to the torsional nature of cutting and turning without large ground reaction forces[13,14]. Alfredson et al. reported significantly higher DXA measured aBMD at the lumbar spine, femoral neck (FN), humerus, distal femur, and proximal tibia in DII female soccer players compared to non-active controls[1]. Likewise, Nikander et al. reported a 19.9% higher weight-, height- and age-adjusted FN aBMD in soccer players compared to nonathletic controls[13]. While there have been a number of studies examining the effects of physical activity on aBMD in many different sports, few have investigated this relationship longitudinally in female soccer players. A study in college female athletes found significant increases in aBMD of the total body, arms and legs from the off- or pre-season to post-season indicating an adaptation to loading over the competitive season[3]; however, an odd-impact loading sport was not represented in the aforementioned study. Additionally, changes in aBMD at a regional site such as the hip were not investigated.
Peripheral quantitative computed tomography (pQCT) provides unique densitometry measures separating cortical and trabecular regions as well as geometric properties of bone, which provide an indication of bone strength. Although DXA studies have demonstrated higher aBMD measures in athletes compared to non-athlete controls, studies using pQCT measures have found lower cortical volumetric BMD (vBMD) in the athlete group compared to controls[6,15-21]. However, these cross-sectional studies find greater cortical area, thickness, and moment of inertia in the athlete groups demonstrating a geometric adaption to exercise[6,15-20]. Additionally, a longitudinal study by Weidauer et al. found significant increases in bone area and cortical thickness at the 20% site of soccer players over 27-31 weeks (including the competitive and off-season periods) showing a positive adaptation to odd-impact loading over time[22].
With the beneficial effect of soccer on aBMD and bone geometry demonstrated in previous studies, it is important to understand how intense, collegiate sport participation effects the body over a season and how this relates to positive bone changes that may continue past the athlete’s career or if additional participation in collegiate athletics perpetuates the positive influence of sports on bone accrual that is seen in adolescence.
The objective of this study was to test the effect of one competitive season and off-season training on lean mass and fat mass changes measured by DXA. Additionally, we investigated the changes in total hip and FN aBMD from pre- to post-season and post- to off-season as well as longitudinal changes in pQCT measures. We hypothesized that over the competitive season lean mass, total hip aBMD, FN aBMD and tibial vBMD would decrease, and tibial bone size would increase. During the off-season, we hypothesized that lean mass, aBMD and vBMD would return to pre-season levels. We further investigated whether or not changes differed by player status (starter vs. non-starter).
Materials and methods
Subjects
The study was approved by the South Dakota State University Institutional Review Board and written informed consent was obtained from each study participant before the study began. Subjects included 24 NCAA Division-I (D-I) female collegiate soccer players and 18 non-athlete controls. Non-athlete controls were female students recruited from campus who exercised no more than 2 days per week for a total of less than 60 minutes/week during the study time frame. Individuals who had been diagnosed with any illness or currently were taking medications known to affect bone metabolism were excluded from the study. For a secondary analysis, the soccer player group was divided into starters (n=11) and non-starters (n=13) based on their mean playing time during the competitive season (top 11 soccer players with ≥70 min/game were defined as starters).
Study procedures
All study participants were asked to complete three study visits. The first visit occurred just prior to the start of the competitive season (August; pre-season). The second visit took place within one week after the completion of the competitive season (November; post-season), and the third visit after the completion of the off-season (May; off-season). Control subjects completed their study visit at the same time intervals as the soccer athletes. Time between the pre-season and post-season visit was approximately 3 months while time between the post-season and off-season visit was approximately 6 months.
Height was measured using a stadiometer (Seca Model 225, Chino, CA) to the nearest 0.5 cm and weight was measured on a digital scale (Seca Model 872, Chino, CA) to the nearest 0.1 kg. Questionnaires including a brief medical history, current health status and medication use, activity patterns, and menstrual status were administered to each participant.
Bone measurements were obtained using two different technologies: DXA and pQCT. Hip and FN aBMD were obtained using DXA (Hologic Discovery; Software version Apex 3.3; Hologic, Inc., Bedford, MA) along with body composition measurements of fat mass, lean mass, and body fat percentage (BF%) using NHANES reference database. The coefficient of variation (CV) for DXA hip aBMD is 1.7%. In this study, the hip of the “kicking leg” was measured as indicated by the participant answering the question, “Which foot do you most often use to kick a ball?” pQCT measurements of the participants’ “kicking leg” were obtained at the 4% and 20% site of the distal tibia (indicating trabecular and cortical measures, respectively) using the Stratec XCT3000 bone densitometer (Orthometrix Inc., Naples, FL) following standard operating procedures. The 20% site was chosen due to the greater amount of physiologic response to physical activity at this distal location which is why tibial stress fractures occur most often in the distal 1/3 of the tibia[23-25]. Tibia length was measured using a segmometer (Rosscraft) as the total distance between the medial tibial condyle and the medial malleolus of the tibia and used to locate image slices. A 30-line scout view was used to reference the distal end of the bone. The settings used to obtain the image were voxel size 0.4 mm and 20 mm/sec scan speed. Contour Mode 2 and Peel Mode 2 were used for the analysis. The density threshold to define trabecular bone (4% slice) was 400 mg/cm3. The density threshold to define cortical bone (20% slice) was 710 mg/cm3. To define the bone edge for pSSI calculation, a density threshold of 280 mg/cm3 was used. The 4% site provided trabecular vBMD. The 20% site provided cortical BMC, cortical vBMD, cortical thickness, cortical area and periosteal circumference. A calculated measure of bone strength, polar strength strain index (pSSI), also was obtained from this site. The CV for trabecular vBMD at the 4% site is 0.5%. The CVs for the 20% site are: cortical BMC, 0.7%; cortical vBMD, 0.4%; cortical thickness, 1.1%; cortical area, 0.8%; and periosteal circumference, 0.5%.
Strength measurements of extension (EPT) and flexion (FPT) peak torque production and hamstring/quadriceps (H/Q) ratio were obtained using isokinetic testing on a Biodex System 4 dynamometer (Biodex Medical Systems, Shirley, NY). Participants were seated with their waist strapped to the chair, the dominant leg knee was located next to the control arm fulcrum, and the participant’s dominant foot was secured to the foot holder with a Velcro strap. The participant completed a series of familiarization reps prior to each test of a different speed. The procedure consisted of 5 repetitions of isokinetic knee extension and flexion at 90, 180, and 360 degree per second bouts with a one-minute rest period between velocities.
Statistics
The differences in baseline subject characteristics between groups were analyzed using t-tests and chi-square analysis. The differences in baseline DXA, pQCT and Biodex measures between groups were analyzed by multiple regression adjusting for baseline height, lean mass, and fat mass. To test differences in mean change in DXA, pQCT, and Biodex outcome measures, a multiple regression analysis was used. All models for DXA and pQCT bone outcomes were adjusted for baseline measures of height, bone, lean mass and fat mass. Biodex and body composition models were adjusted for concomitant baseline measure, baseline height, lean mass and fat mass. Marginal mean change within groups was tested to determine a difference from zero. A secondary analysis was performed dividing the soccer player group into starters and non-starters based on playing time (described above). All tests were considered significant at p<0.05.
Results
Pre-season to post-season
Subject characteristics
Unadjusted baseline characteristics are presented in Table 1. At the pre-season visit, control subjects were older, taller and heavier than soccer players (all, p<0.05). Baseline weight, fat mass and body fat percent were lower in soccer athletes than controls (all, p<0.01). Forty-four percent of controls and 46% of soccer players were currently using hormonal contraceptives (p=0.93). Irregular menstrual status determined by self-report of not menstruating every 21-35 days occurred in 22% of controls and 33% of soccer players (p=0.43).
Table 1.
Pre-season descriptive characteristics of the groups.
| Variable | Controls (n=18) | Soccer Players (n=24) | p-value |
|---|---|---|---|
| Age (yr) | 20±0.4 | 19±0.2 | 0.03 |
| Height (cm) | 169±1.1 | 165±1.3 | 0.04 |
| Weight (kg) | 73±2.1 | 64±1.5 | <0.01 |
| Body Fat (%) | 29±1.0 | 22±0.7 | <0.01 |
| Fat Mass (kg) | 22±1.3 | 14±0.8 | <0.01 |
| Lean Mass (kg) | 50±1.0 | 48±0.9 | 0.17 |
| Current Contraceptive Use (%) | 44 | 46 | 0.93 |
| Irregular Menstrual Status (%) | 22 | 33 | 0.43 |
Values are unadjusted means±SD.
Pre-season baseline measurements
Group differences in unadjusted and adjusted baseline outcome measures are presented in Table 2. None of the unadjusted DXA aBMD measures were different between groups, but total hip and FN aBMD were higher in soccer players in models adjusting for baseline height, lean mass, and fat mass (p=0.01 and p=0.04; respectively). Unadjusted trabecular vBMD was greater in soccer players at baseline, but this effect did not remain significant in adjusted models. There were no other differences in baseline pQCT measures between groups. Unadjusted EPT measures were not different between groups. In the adjusted models, EPT at 90°/sec was greater in soccer players than controls. FPT measures at all speeds were greater in soccer players than controls before and after adjustments with the exception of adjusted FPT at 360°/sec. H/Q ratio at all speeds was higher in soccer players than controls but only remained different at 180°/sec in adjusted models.
Table 2.
Pre-season baseline DXA, pQCT and Biodex measures.
| Control | Soccer Players | p-value | Adj. p-value | |
|---|---|---|---|---|
| Bone Measurements: | n=18 | n=24 | ||
| DXA | ||||
| Hip BMC (g) | 36.6±1.1 | 37.0±1.0 | 0.76 | 0.41 |
| Hip aBMD (g/cm2) | 1.07±0.0 | 1.13±0.0 | 0.10 | 0.01 |
| FN BMC (g) | 4.9±0.2 | 5.0±0.1 | 0.90 | 0.17 |
| FN aBMD (g/cm2) | 1.00±0.0 | 1.02±0.0 | 0.63 | 0.04 |
| pQCT: 4% Trabecular site | ||||
| Trab vBMD (mg/cm3) | 260.5±7.4 | 283.8±5.6 | 0.01 | 0.22 |
| pQCT: 20% Cortical Site | ||||
| vBMD (mg/cm3) | 1163.0±4.7 | 1160.3±3.3 | 0.62 | 0.59 |
| BMC (g) | 258.2±6.0 | 256.1±5.4 | 0.79 | 0.55 |
| Bone area (mm2) | 222.2±5.4 | 220.7±4.5 | 0.83 | 0.58 |
| Thickness (mm) | 3.8±0.1 | 4.0±0.1 | 0.29 | 0.70 |
| Periosteal circumference (mm) | 70.5±1.1 | 68.2±0.9 | 0.11 | 0.31 |
| pSSI (mm3) | 1582.2±51.6 | 1477.9±47.1 | 0.15 | 0.37 |
| Strength Measurements: | n=18 | n=23 | ||
| Biodex: Extension Peak Torque | ||||
| 90 °/sec | 101.9±4.4 | 105.0±3.3 | 0.56 | 0.03 |
| 180 °/sec | 76.7±3.5 | 79.2±2.5 | 0.57 | 0.07 |
| 360 °/sec | 51.8±2.6 | 52.2±2.2 | 0.91 | 0.26 |
| Biodex: Flexion Peak Torque | ||||
| 90 °/sec | 46.5±2.4 | 58.2±2.9 | <0.01 | 0.03 |
| 180 °/sec | 36.1±1.9 | 44.8±2.0 | <0.01 | 0.02 |
| 360 °/sec | 24.8±1.5 | 30.1±1.6 | 0.02 | 0.13 |
| Biodex: Hamstring/Quadriceps Ratio | ||||
| 90 °/sec | 46.0±2.0 | 55.8±2.5 | <0.01 | 0.20 |
| 180 °/sec | 47.0±1.3 | 56.6±1.9 | <0.01 | 0.05 |
| 360 °/sec | 47.8±1.4 | 59.0±2.8 | <0.01 | 0.15 |
All values are expressed as unadjusted means±SD. One baseline Biodex test in the soccer group was not used due to improper test completion. Adjusted p-value controls for baseline height, lean mass and fat mass. DXA, dual-energy x-ray absorptiometry; BMC, bone mineral content; aBMD, areal bone mineral density; FN, femoral neck; pQCT, peripheral quantitative computed tomography; vBMD, volumetric bone mineral density; pSSI, polar strength strain index.
Pre-season to post-season changes
Two individuals did not complete a post-season visit and were excluded from the outcome change analysis (soccer, n=23; control, n=17).
Body Composition: There were no differences in lean or fat mass change between soccer players and controls. However, soccer players lost lean mass (1.7%) from pre- to post-season (p<0.01; Figure 1A), but this loss of lean mass was significant only in non-starters (-1.2±0.3 kg; p<0.01; data not shown).
Figure 1.
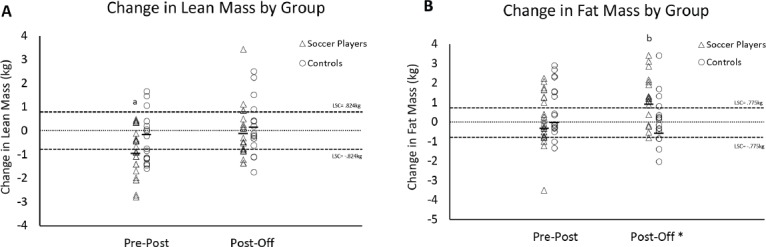
DXA measured changes in lean mass (Panel A) and fat mass (Panel B) from pre- to post-season and from post- to off-season by group. The letter a indicates a significant change in the group mean from pre- to post-season, while the letter b indicates a significant change in the group mean from post- to off-season. LSC = least significant change. Horizontal lines are adjusted group marginal mean changes. *There was a significant difference in fat mass mean change between the soccer players and the control group from post- to off-season (p≤0.05).
DXA: From pre- to post-season, control subject FN and hip aBMD increased (all, p<0.03), while no change was observed in soccer players (Figure 2A & 2B). Mean change in FN aBMD was different between the soccer players and controls (p=0.02). Change in hip aBMD was not different between groups. Change in FN aBMD in non-starters and starters was different from controls (0.002±0.008 g/cm2 and -0.005±0.01 g/cm2 vs. 0.029±0.008 g/cm2, respectively; both p<0.04) but not each other (p=0.53). Adding change in lean mass to the models did not alter results.
Figure 2.

Changes in total hip (Panel A) and femoral neck aBMD (Panel B) from pre- to post-season and from post- to off-season by group. The letter a indicates a significant change in the group mean from pre- to post-season, while the letter b indicates a significant change in the group mean from post- to off-season. Horizontal lines are adjusted group marginal mean changes. LSC = least significant change. *There was a significant difference in the FN aBMD mean change between the soccer players and the control group from pre- to post-season (p<0.05).
pQCT: At the 4% trabecular site, there were no differences between groups or changes in trabecular vBMD (Figure 3A). At the 20% cortical site, there were increases in the soccer players in cortical BMC and cortical area similar to that observed for periosteal circumference (Figure 3B), and the mean changes were different from controls (all, p≤0.05). Cortical BMC and bone area increased in both starter and non-starter groups, which were different from controls (all; p<0.04) but not each other (BMC, 4.2±1.8 and 3.0±1.4 vs. -1.3±1.4g, respectively; both p<0.05; Area, 3.6±1.5 and 2.5±1.1 vs. -0.9±1.1 mm2, respectively; both p<0.05). Periosteal circumference increased in the starter group (0.5±0.2 mm, p=0.04), which was not different from controls or non-starters (p=0.09 and p=0.58, respectively). There were no changes or differences between groups in cortical vBMD, thickness, and pSSI.
Figure 3.

Changes in trabecular vBMD (Trab vBMD, Panel A), periosteal circumference (Peri C, Panel B), cortical thickness (Panel C), cortical vBMD (Panel D), and pSSI (Panel E) from pre- to post-season and from post- to off-season by group. The letter a indicates a significant change in the group mean from pre- to post-season, while the letter b indicates a significant change in the group mean from post- to off-season. Horizontal lines are adjusted group marginal mean changes. LSC= least significant change. *There was a significant difference in periosteal circumference mean change between the soccer player group and the control group from pre- to post-season (p<0.05).
Strength: Control subjects increased their FPT at 180°/s (p<0.01), but this change was not different from soccer players (Figure 4A). Soccer players increased FPT at 360°/s (p<0.01), but this was not different from the control group (Figure 4B). Only the starter group showed an increase in FPT at 180°/s (3.7±1.8 ft-lbs, p=0.04) and 360°/s (5.1±2.0 ft-lbs, p=0.01). The increase observed in starters at 180°/s and 360°/s was not different from non-starters, but the increase at 360°/s was different from controls (-1.0±1.6 ft-lbs, p=0.04). The results did not change when peak torque was normalized to body weight. Change in lean mass did not explain changes in strength.
Figure 4.

Changes in peak torque at 180°/s (FPT 180, Panel A), peak torque at 360°/s (FPT 360, Panel B), hamstring/quadriceps ratio at 180°/s (H/Q 180, Panel C), and hamstring/quadriceps ratio at 360°/s (H/Q 360, Panel D) from pre- to post-season and from post- to off-season by group. The letter A indicates a significant change in the group mean from pre- to post-season, while the letter B indicates a significant change in the group mean from post- to off-season. Horizontal lines are adjusted group marginal mean changes. Least significant changes for Biodex measurements are not available.
H/Q ratio increased at the 180°/s measure in controls but was not different from soccer players (Figure 4C). Soccer players increased H/Q ratio at 360°/s, but this was not different from controls (Figure 4D). Only the starter group increased H/Q ratio at 360°/s (7.5±3.0, p=0.01) which was not different from non-starters (2.6±2.6, p=0.22) or controls (-0.8±2.4, p=0.07). Change in lean mass did not explain changes in H/Q ratio.
Post-season to off-season
Subject characteristics
All baseline measures that were different between groups at the pre-season visit remained different at the post-season visit except current hormonal contraceptive use. Seventy-one percent (12/17) of controls and 39% (9/23) of soccer players were using hormonal contraceptives at the post-season visit (p<0.05).
Post-season baseline measurements
Post-season baseline measurements in each group are presented in Table 3. No DXA outcomes, unadjusted or adjusted, were different between groups. Trabecular vBMD was higher in the soccer player group but did not remain significant after adjusting for covariates. No other unadjusted or adjusted pQCT measures were different between groups. FPT at 360°/sec was higher in soccer players, but this did not remain significant when adjusted for post-season baseline height, lean mass and fat mass. H/Q ratio was greater in soccer players at speeds of 180 and 360°/sec but did not remain so after adjustments.
Table 3.
Post-season baseline DXA, pQCT and Biodex measures.
| Control | Soccer Players | p-value | Adj. p-value | |
|---|---|---|---|---|
| Bone Measurements: | n=17 | n=23 | ||
| DXA | ||||
| Hip BMC (g) | 37.8±1.1 | 37.3±1.1 | 0.75 | 0.78 |
| Hip aBMD (g/cm2) | 1.09±0.0 | 1.13±0.0 | 0.16 | 0.09 |
| FN BMC (g) | 5.1±0.2 | 5.0±0.1 | 0.76 | 0.53 |
| FN aBMD (g/cm2) | 1.03±0.0 | 1.03±0.0 | 0.95 | 0.28 |
| pQCT: 4% Trabecular Site | n=16 | n=22 | ||
| vBMD (mg/cm3) | 260.5±7.4 | 283.8±5.6 | 0.01 | 0.14 |
| pQCT: 20% Cortical Site | ||||
| BMC (g) | 257.2±6.1 | 260.6±5.8 | 0.70 | 0.95 |
| vBMD (mg/cm3) | 1160.7±4.1 | 1160.9±3.5 | 0.97 | 0.88 |
| Bone area (mm2) | 221.7±5.6 | 224.3±4.6 | 0.72 | 0.93 |
| Thickness (mm) | 3.7±0.1 | 4.0±0.1 | 0.14 | 0.50 |
| Periosteal circumference (mm) | 70.6±1.1 | 68.7±0.9 | 0.19 | 0.47 |
| pSSI (mm3) | 1590.1±57.9 | 1490.9±51.6 | 0.21 | 0.47 |
| Strength Measurements: | n=17 | n=23 | ||
| Biodex: Extension Peak Torque | ||||
| 90 °/sec | 103.6±4.5 | 104.8±3.1 | 0.82 | 0.26 |
| 180 °/sec | 79.1±3.6 | 80.2±2.4 | 0.81 | 0.13 |
| 360 °/sec | 52.5±3.2 | 51.6±2.1 | 0.81 | 0.51 |
| Biodex: Flexion Peak Torque | ||||
| 90 °/sec | 52.2±2.9 | 57.9±1.8 | 0.08 | 0.37 |
| 180 °/sec | 41.6±2.2 | 46.5±1.8 | 0.09 | 0.56 |
| 360 °/sec | 26.1±1.8 | 31.7±1.5 | 0.02 | 0.09 |
| Biodex: Hamstring/Quadriceps Ratio | ||||
| 90 °/sec | 50.9±2.3 | 55.5±1.2 | 0.06 | 0.84 |
| 180 °/sec | 53.0±2.0 | 58.0±1.5 | 0.04 | 0.53 |
| 360 °/sec | 50.1±2.4 | 61.4±1.9 | <0.01 | 0.12 |
All values are expressed as unadjusted means±SD. Two subjects did not complete a post-season study visit. Two post-season pQCT scans were not analyzed due to scanning error. Adjusted p-value controls for baseline height, lean mass and fat mass. DXA, dual-energy x-ray absorptiometry; BMC, bone mineral content; aBMD, areal bone mineral density; FN, femoral neck; pQCT, peripheral quantitative computed tomography; vBMD, volumetric bone mineral density; pSSI, polar strength strain index.
Post-season to off-season changes
One soccer player transferred and one control subject increased physical activity above the study criteria and was excluded from further analysis. Four senior soccer players did not participate in spring season training and were excluded from the post-season to off-season analysis (soccer, n=18; control, n=16).
Body Composition: There were no changes or differences between groups in lean mass. Soccer players gained fat mass (~8.0%), and this gain was different from controls (p=0.01; Figure 1B). Fat mass change was significant in starters (1.8±0.5 kg; p<0.01) and approached significance in non-starters (1.1±0.6 kg; p=0.06) with the change in the starter group different from the control group but not the non-starter group. There were no changes or differences between groups in lean mass.
DXA: Total hip and FN aBMD decreased in controls (both p≤0.05; Figures 2A & 2B). These mean changes were not different from the soccer players. Adding changes in lean mass or fat mass did not explain changes in aBMD. There were no significant changes in aBMD in the starter and non-starter groups.
pQCT: Trabecular vBMD significantly decreased in soccer players (p=0.02), but this change was not different from the change in controls (p=0.31; Figure 3A). Within the soccer player group, there was no difference in change in trabecular vBMD between starters and non-starters. Change in lean mass did not affect trabecular vBMD results.
At the 20% site, cortical BMC and cortical area increased in both soccer players and controls similar to that shown for thickness (all p<0.01, Figure 3C), and these changes were not different between groups. Additionally, cortical vBMD (p<0.01) and pSSI (p<0.01, Figures 3D & 3E) increased in the control group, but the change was not different from the change in the soccer players. Both the starter and non-starter groups had increases in cortical BMC and cortical area that were not different from each other or the controls (data not shown); whereas, only starters increased cortical thickness and approached a significant increase in pSSI (p=0.07). The mean changes in the starters were not different from non-starters or controls. Adding change in lean mass or current hormonal contraceptive use did not alter any aforementioned results.
Strength: Controls decreased FPT (p=0.05) at 360°/s, but the change in FPT was not different from soccer players (p=0.25; Figure 4B). There were no changes in any of the strength measures in the soccer player group. The starter group of soccer players increased EPT at 90°/s (9.5±3.2 ft-lbs; p<0.01) which was different from non-starters (-1.1±2.6 ft-lbs; p=0.01) but not controls (1.5±2.3 ft-lbs; p=0.09). The mean change in EPT at 360°/s for the starter group was different from the non-starter group (5.9±3.7 ft-lbs vs. -4.3±2.9 ft-lbs, p=0.03) and approached a significant difference from the control group (-4.2±2.5 ft-lbs, p=0.06). There were no differences among or between the starter and non-starter groups for FPT measures. Adding change in lean mass did not affect results.
There were no changes or differences in H/Q ratio between the soccer player and control groups (Figures 4C & 4D). However, the starter group decreased their H/Q ratio at 360°/s (-9.8±4.5, p=0.03) which was different from non-starters (5.8±3.6, p<0.01) but not controls. Change in lean mass did not remain in the model for H/Q ratio results.
Discussion
Throughout the entire soccer season (pre-season to off-season), the soccer players experienced significant changes in body composition, bone geometry and strength. The soccer players lost lean mass during the 3-month long competitive season and gained fat mass from the post-season to off-season measure (~6 months). This did not translate to a decrease in or increase in aBMD at any time point. However, tibia bone size increased pre-to post-season while cortical thickness increased from post-season to off-season. The decrease in lean mass during the competitive season did not result in a decrease in strength, rather, the soccer players increased FPT at the highest speed (360°/s) as well as H/Q ratio at the same speed.
Body composition
In our study, soccer players lost significant lean mass (particularly in the non-starter group) over the competitive season while gaining fat mass over the 6-month off-season training period. Although the change in the soccer group was not different from the control group, this is a significant clinical finding which requires further investigation. While some studies have reported a maintenance or even gain of lean mass from pre- to post-season in various sports such as soccer, softball, track, swimming, basketball and volleyball[3,5,7,22,26-28]; other studies have reported losses in lean mass from pre- to post-season in basketball, rugby and soccer athletes[3,4,9,29-31]. The loss of lean mass (and gain in BF%) over the competitive season seen in our study may be attributed to the change in the strength program. The soccer players participated in 3 days per week of required strength training prior to the start of the competitive season and only one day per week of strength training during the competitive season. As the loss of lean mass was only significant in non-starters, we also may attribute the lack of playing time in games as a possible contributor to the loss of lean mass. Non-starters averaged 12 minutes/game while starters averaged 77 minutes/game, which resulted in a difference of 19.5 hours of playing time over the 3-month time period. Another reason for the decrease in lean mass could be a negative energy balance, but participants were non-compliant in completing dietary questionnaires; therefore, we do not have sufficient data to test this hypothesis. Contradictory to our hypothesis, soccer players did not regain lean mass from the post-season to off-season visit but gained a significant amount of fat mass. The reasoning behind this result is difficult to ascertain as no other studies have looked at this particular time period; just after the completion of the competitive season to the end of the off-season training period (not including the 3 months of summer training just prior to pre-season). There is approximately a 2-week period after the completion of the competitive season where the athletes were not asked to complete any mandatory strength and conditioning workouts. Otherwise, strength workouts were assigned for the holiday break (~one month) when the athletes are at home. Therefore, the amount of time allotted for a possible detraining effect to allow for significant fat gain seems improbable. The authors speculate that it may be related to a decrease in training intensity and/or volume. Even though the strength training returns to 3 days a week (as it was just before pre-season), the intensity may not be the same. Also, the team was practicing 4 days/week and competed in 18 total games during the competitive season whereas the off-season practices are 4 days/week with ~7 total games, which is a decrease in total training volume. Again, there was insufficient dietary data to analyze for its potential role in energy balance during the off-season. Future studies should include measures of training intensity to determine its role on changes in body composition throughout the competitive and off seasons.
DXA bone density
Our study assessed longitudinal changes in DXA measures over the competitive season and off-season of D-I female soccer players. Contradictory to our hypothesis, there were no changes in bone measures in the athletes in either the pre- to post-season or post- to off-season time frame. However, the control subjects did increase total hip and FN aBMD (with no change in total hip and FN area) over the pre- to post-season time frame, but this was not different from the soccer players. The increase in FN aBMD was the only measure different from the soccer player group. Adding change in moderate-vigorous activity and contraceptive use to the model did not change the pre-season to post-season results in the control group. Our results differ from another study of female athletes that demonstrated softball, basketball, volleyball and track and field athletes significantly increased total body, arms and legs aBMD over the competitive season (~12 weeks). These increases indicate an adaptation to loading over the competitive season which was not seen in our study[3]. Conversely, Stanforth et al. found no change leg, arm, pelvis, spine and trunk aBMD in female soccer athletes from pre-season to post-season[32]. Soccer is an odd-impact loading sport which may yield different results compared to high- and low-impact loading sports due to sport-specific loading patterns. Although a gain in aBMD was not expected, we are pleased to see that even though soccer player group did lose lean mass, this did not correlate to a loss of aBMD.
The controls decreased FN and hip aBMD from post-season to off-season (~6 months) with none of these changes different from the soccer player group. Unfortunately, we did not have vitamin D status or calcium intake data to determine if low vitamin D status or low calcium intakes during the winter season played a factor in the bone loss seen in the controls. A study by Taaffe et al. reported an increased percent change in DXA measured spine and FN aBMD in gymnasts compared to runners, swimmers and controls over a period of 8 to 12 months. These investigators reported a greater influence on change in aBMD of a high-impact loading sport (gymnastics) than a low- (running) or active (swimming) loading sport as well as non-active controls[9]. The time between our post-season and off-season visit was approximately 6 months which provides ample time to see bone adaptations should they occur. However, another study found no change in aBMD in female soccer athletes from post-season to the following pre-season even though all other sports measured (volleyball, basketball, swimming and track/field) demonstrated one or more changes over the same time period[32]. The only change seen in the soccer group was a 1.2% increase in leg BMD from the first-year pre-season to the third-year post-season suggesting a long-term bone adaption over the course of the athlete’s career[32]. It is unknown whether it is the nature of the odd-impact loading of the sport of soccer or the type of year-round training of the sport that produces consistent measures of total hip and FN aBMD at various time points in the collegiate training environment.
pQCT bone density and geometry
Over the competitive season, soccer players significantly increased cortical BMC and cortical area by 1.4%, and periosteal circumference by 0.6%, and these changes were different from controls. The increase in periosteal circumference supported our hypothesis of increased bone size over the competitive season. Our results are similar to another longitudinal study which demonstrated an increase in cortical bone area and thickness in female soccer players from the pre-season to off-season visit compared to non-active controls[22]. This increase in bone size suggests an adaptation to the increase in loading experienced during the competitive season training as well as the osteogenic type of odd-impact loading experienced in sports like soccer and tennis[14,18,19]. Additionally, an increase in bone size was only significant in the starter group that experienced a greater amount of playing time throughout the season. Bone will adapt to the loads placed upon it and can alter its shape based on those types of loads[33,34]. Weidauer et al.[6] and Rantalainen et al.[18] demonstrated that different types of sports affect pQCT measured tibial geometry based on sport-specific loading. Additionally, a rather important limitation to note about this study is the use of the dominant “kicking” leg for all pQCT measures. Although soccer athletes are expected to be proficient at utilizing both legs within the competitive environment, it has been shown that differences between the kicking leg and support leg occur in elite athletes due to the unique forces experienced by each limb during the kicking movement pattern[35]. It is unknown whether or not the changes seen in the pQCT measures of this study would be different if they had been measured in the support leg. In the soccer athletes in our study, the increase in training results in circumferential growth to resist the unfamiliar microstrains placed on the bone; however, this did not translate to an increase in calculated bone strength as measured by pSSI. Additionally, from the pre- to post-season measure, we did not see the decrease in cortical vBMD due to increased remodeling as we hypothesized. We did see a 7.5% increase in cortical BMC, attributed to a 2.6% increase in area and a 3.1% increase in thickness from the post- to off-season measure with no gain in cortical vBMD in the soccer players; however, this was not different from the control group. Again, the increase in cortical thickness was significant in the starter group only indicating a potential effect of greater playing time in competitions and perhaps, training intensity during practices. The increased cortical thickness is due to endosteal contraction and could represent the remodeling and repairing phase when the bone has the appropriate rest periods to adapt the mechanical properties by mineralizing newly formed osteoid in response to the loads experienced during the competitive season. This represents the importance of rest periods to allow the bone to make the appropriate changes to its mechanical and geometrical structure before damage; and thus injury, could occur.
Strength
Collegiate level soccer demands skill in quickness, speed, sprinting, jumping/heading, rapid acceleration and deceleration, balance and changing direction at varying speeds and intensities. These activities require the proper level of strength and power for an overall effective performance. Few studies have investigated strength in female soccer players and how it is related to changes in bone and performance measures such as kicking velocity and ball velocity while there have been studies for male counterparts[36-38]. A study by Brophy et al. demonstrated that the muscle activation and biomechanics during a soccer kick of a male versus a female differs greatly; therefore, strength performances of male and female soccer players need to be examined separately[39]. A recent study of 22 D1 female soccer players measured knee and hip torque on a Biodex isokinetic dynamometer[40]. They reported knee torque to be correlated with ball velocity (a measure used to assess kicking performance)[40]. Although this study performed pre- and post-season measures, they did not report whether or not there were strength changes over the competitive season and into the off-season. Our study found some changes in strength over the competitive season. Soccer players increased FPT at the 360°/s measure. This correlated with the increase in H/Q ratio of soccer players at the same speed measure as an increase in flexion peak torque indicates an increase in hamstring strength; thus, improving the ratio of quadriceps to hamstring strength ratio. Only the starter group, not the non-starter group, saw increases in FPT at the 180 and 360°/s measures which may indicate an effect of playing time on hamstring strength gains at higher speeds. This may be an effect of velocity-specific training suggested by Coyle et al.[41] who showed that training at lower velocities only increases strength at lower velocities (i.e. 60°/s), but training at higher velocities (180 and 300°/s) increases strength at low and high velocities. Even though the soccer players experienced a decrease in lean mass over the competitive season, this did not translate to a decrease in extension or flexion peak torque at the knee or a decrease in H/Q ratio. During the off-season, the group of starters increased extension peak torque at 90°/s (which was different from non-starters), and the change in EPT at 360°/s in starters was greater than non-starters. Additionally, the gain in H/Q ratio at the 360°/s measure that occurred in the starters over the competitive season was lost over the off-season training. This knowledge is beneficial in examining the effect of the season (both competitive and off-season) and playing status (starter or non-starter) on changes in strength which may provide valuable information for changes in performance measures, adjustments to training protocols (training at higher speeds to increase hamstring strength at sport-specific speeds) and the role of quadriceps/hamstrings ratio (H/Q) in anterior cruciate ligament (ACL) injuries in female soccer players.
Conclusion
The soccer players in this study lost lean mass over the competitive season and gained fat mass but did not recover lean mass in the off-season. Although this did not translate to a decrease in strength measures, the loss of lean mass could be a sign of a negative outcome related to overtraining or negative energy balance which should be assessed in future studies. Bone density measures did not change over the entire study timeframe; however, we did find there was an increase in periosteal circumference from pre- to post-season and cortical thickness in the off-season in soccer players. Interestingly, these geometrical changes were significant in the starter group (not the non-starter group) indicating a possible effect of playing time in competitions and perhaps, training intensity during practices. The female soccer athlete experiences significant changes in body composition and bone geometry which differ depending on the time frame studied: the competitive season (3 months) and off-season (6 months) and on the athlete’s playing status. It is important to understand that cross-sectional evaluations of these athletes may not capture the whole picture of the seasonal training effect of collegiate sports. Certain training techniques and practices may have positive or negative consequences on athlete’s health that may or may not be overtly apparent (such as changes in lean mass or bone). It is important evaluate athletes at key time points across the full training season to optimize overall health and performance and decrease risk of future injury.
Acknowledgements
The author acknowledges the Ethel Austin Martin Endowed Program in Human Nutrition at South Dakota State University for the support of this project.
Footnotes
The authors have no conflict of interest.
Edited by: A. Ireland
References
- 1.Alfredson H, Nordstrom P, Lorentzon R. Total and regional bone mass in female soccer players. Calcif Tissue Int. 1996;59:438–42. doi: 10.1007/BF00369207. [DOI] [PubMed] [Google Scholar]
- 2.Alfredson H, Nordstrom P, Lorentzon R. Bone mass in female volleyball players: a comparison of total and regional bone mass in female volleyball players and nonactive females. Calcif Tissue Int. 1997;60:338–42. doi: 10.1007/s002239900239. [DOI] [PubMed] [Google Scholar]
- 3.Carbuhn AF, Fernandez TE, Bragg AF, Green JS, Crouse SF. Sport and training influence bone and body composition in women collegiate athletes. Journal of Strength & Conditioning Research (Lippincott Williams & Wilkins) 2010;24:1710–7. doi: 10.1519/JSC.0b013e3181d09eb3. [DOI] [PubMed] [Google Scholar]
- 4.Miller TA, Thierry-Aguilera R, Congleton JJ, et al. Seasonal changes in VO2max among Division 1A collegiate women soccer players. J Strength Cond Res. 2007;21:48–51. doi: 10.1519/00124278-200702000-00009. [DOI] [PubMed] [Google Scholar]
- 5.Stanforth PR, Crim BN, Stanforth D, Stults-Kolehmainen MA. Body composition changes among female NCAA division 1 athletes across the competitive season and over a multiyear time frame. J Strength Cond Res. 2014;28:300–7. doi: 10.1519/JSC.0b013e3182a20f06. [DOI] [PubMed] [Google Scholar]
- 6.Weidauer LA, Eilers MM, Binkley TL, Vukovich MD, Specker BL. Effect of different collegiate sports on cortical bone in the tibia. J Musculoskelet Neuronal Interact. 2012;12:68–73. [PubMed] [Google Scholar]
- 7.Clark M, Reed DB, Crouse SF, Armstrong RB. Pre- and post-season dietary intake, body composition, and performance indices of NCAA division I female soccer players. Int J Sport Nutr Exerc Metab. 2003;13:303–19. doi: 10.1123/ijsnem.13.3.303. [DOI] [PubMed] [Google Scholar]
- 8.Fehling PC, Alekel L, Clasey J, Rector A, Stillman RJ. A comparison of bone mineral densities among female athletes in impact loading and active loading sports. Bone. 1995;17:205–10. doi: 10.1016/8756-3282(95)00171-9. [DOI] [PubMed] [Google Scholar]
- 9.Taaffe DR, Robinson TL, Snow CM, Marcus R. High-impact exercise promotes bone gain in well-trained female athletes. J Bone Miner Res. 1997;12:255–60. doi: 10.1359/jbmr.1997.12.2.255. [DOI] [PubMed] [Google Scholar]
- 10.Heinonen A, Oja P, Kannus P, et al. Bone mineral density in female athletes representing sports with different loading characteristics of the skeleton. Bone. 1995;17:197–203. doi: 10.1016/8756-3282(95)00151-3. [DOI] [PubMed] [Google Scholar]
- 11.Heinonen A, Oja P, Kannus P, Sievanen H, Manttari A, Vuori I. Bone mineral density of female athletes in different sports. Bone Miner. 1993;23:1–14. doi: 10.1016/s0169-6009(08)80086-4. [DOI] [PubMed] [Google Scholar]
- 12.Proctor KL, Adams WC, Shaffrath JD, Van Loan MD. Upper-limb bone mineral density of female collegiate gymnasts versus controls. Med Sci Sports Exerc. 2002;34:1830–5. doi: 10.1097/00005768-200211000-00021. [DOI] [PubMed] [Google Scholar]
- 13.Nikander R, Sievanen H, Heinonen A, Kannus P. Femoral neck structure in adult female athletes subjected to different loading modalities. J Bone Miner Res. 2005;20:520–8. doi: 10.1359/JBMR.041119. [DOI] [PubMed] [Google Scholar]
- 14.Ireland A, Degens H, Ganse B, Maden-Wilkinson TM, Wilks DC, Rittweger J. Greater tibial bone strength in male tennis players than controls in the absence of greater muscle output. Journal of Orthopaedic Translation. 2015;3:142–51. doi: 10.1016/j.jot.2015.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Liu L, Maruno R, Mashimo T, et al. Effects of physical training on cortical bone at midtibia assessed by peripheral QCT. J Appl Physiol. 2003;95:219–24. doi: 10.1152/japplphysiol.01055.2002. [DOI] [PubMed] [Google Scholar]
- 16.Nikander R, Kannus P, Rantalainen T, et al. Cross-sectional geometry of weight-bearing tibia in female athletes subjected to different exercise loadings. Osteoporos Int. 2010;21:1687–94. doi: 10.1007/s00198-009-1101-0. [DOI] [PubMed] [Google Scholar]
- 17.Heinonen A, Sievanen H, Kannus P, Oja P, Vuori I. Site-specific skeletal response to long-term weight training seems to be attributable to principal loading modality: a pQCT study of female weightlifters. Calcif Tissue Int. 2002;70:469–74. doi: 10.1007/s00223-001-1019-9. [DOI] [PubMed] [Google Scholar]
- 18.Rantalainen T, Nikander R, Heinonen A, Suominen H, Sievanen H. Direction-specific diaphyseal geometry and mineral mass distribution of tibia and fibula: a pQCT study of female athletes representing different exercise loading types. Calcif Tissue Int. 2010;86:447–54. doi: 10.1007/s00223-010-9358-z. [DOI] [PubMed] [Google Scholar]
- 19.Nikander R, Sievanen H, Uusi-Rasi K, Heinonen A, Kannus P. Loading modalities and bone structures at nonweight-bearing upper extremity and weight-bearing lower extremity: a pQCT study of adult female athletes. Bone. 2006;39:886–94. doi: 10.1016/j.bone.2006.04.005. [DOI] [PubMed] [Google Scholar]
- 20.Haapasalo H, Kontulainen S, Sievanen H, Kannus P, Jarvinen M, Vuori I. Exercise-induced bone gain is due to enlargement in bone size without a change in volumetric bone density: a peripheral quantitative computed tomography study of the upper arms of male tennis players. Bone. 2000;27:351–7. doi: 10.1016/s8756-3282(00)00331-8. [DOI] [PubMed] [Google Scholar]
- 21.Rantalainen T, Nikander R, Daly RM, Heinonen A, Sievanen H. Exercise loading and cortical bone distribution at the tibial shaft. Bone. 2011;48:786–91. doi: 10.1016/j.bone.2010.11.013. [DOI] [PubMed] [Google Scholar]
- 22.Weidauer L, Minett M, Negus C, et al. Odd-impact loading results in increased cortical area and moments of inertia in collegiate athletes. Eur J Appl Physiol. 2014;114:1429–38. doi: 10.1007/s00421-014-2870-5. [DOI] [PubMed] [Google Scholar]
- 23.Jones BH, Thacker SB, Gilchrist J, Kimsey CD, Jr, Sosin DM. Prevention of lower extremity stress fractures in athletes and soldiers: a systematic review. Epidemiol Rev. 2002;24:228–47. doi: 10.1093/epirev/mxf011. [DOI] [PubMed] [Google Scholar]
- 24.Beck TJ, Ruff CB, Mourtada FA, et al. Dual-energy X-ray absorptiometry derived structural geometry for stress fracture prediction in male U.S. Marine Corps recruits. J Bone Miner Res. 1996;11:645–53. doi: 10.1002/jbmr.5650110512. [DOI] [PubMed] [Google Scholar]
- 25.Franklyn M, Oakes B, Field B, Wells P, Morgan D. Section modulus is the optimum geometric predictor for stress fractures and medial tibial stress syndrome in both male and female athletes. Am J Sports Med. 2008;36:1179–89. doi: 10.1177/0363546508314408. [DOI] [PubMed] [Google Scholar]
- 26.Carling C, Orhant E. Variation in body composition in professional soccer players: interseasonal and intraseasonal changes and the effects of exposure time and player position. J Strength Cond Res. 2010;24:1332–9. doi: 10.1519/JSC.0b013e3181cc6154. [DOI] [PubMed] [Google Scholar]
- 27.Silvestre R, Kraemer WJ, West C, et al. Body composition and physical performance during a National Collegiate Athletic Association Division I men’s soccer season. J Strength Cond Res. 2006;20:962–70. doi: 10.1519/R-18165.1. [DOI] [PubMed] [Google Scholar]
- 28.Milanese C, Cavedon V, Corradini G, De Vita F, Zancanaro C. Seasonal DXA-measured body composition changes in professional male soccer players. J Sports Sci. 2015;33:1219–28. doi: 10.1080/02640414.2015.1022573. [DOI] [PubMed] [Google Scholar]
- 29.Kraemer WJ, French DN, Paxton NJ, et al. Changes in Exercise Performance and Hormonal Concentrations Over a Big Ten Soccer Season in Starters and Nonstarters. Journal of Strength & Conditioning Research (Allen Press Publishing Services Inc) 2004;18:121–8. doi: 10.1519/1533-4287(2004)018<0121:ciepah>2.0.co;2. [DOI] [PubMed] [Google Scholar]
- 30.Harley JA, Hind K, O’Hara JP. Three-Compartment Body Composition Changes in elite Rugby League Players During a Super League Season, Measured by Dual-Energy X-ray Absorptiometry. The Journal of Strength & Conditioning Research. 2011;25:1024–9. doi: 10.1519/JSC.0b013e3181cc21fb. 10.519/JSC. 0b013e3181cc21fb. [DOI] [PubMed] [Google Scholar]
- 31.Lees MJ, Oldroyd B, Jones B, et al. Three-Compartment Body Composition Changes in Professional Rugby Union Players Over One Competitive Season: A Team and Individualized Approach. J Clin Densitom. 2016:1–8. doi: 10.1016/j.jocd.2016.04.010. [DOI] [PubMed] [Google Scholar]
- 32.Stanforth D, Lu T, Stults-Kolehmainen MA, Crim BN, Stanforth PR. Bone mineral content and density among female NCAA Division I athletes across the competitive season and over a multi-year time frame. J Strength Cond Res. 2014 doi: 10.1519/JSC.0000000000000785. [DOI] [PubMed] [Google Scholar]
- 33.Frost HM. The mechanostat: a proposed pathogenic mechanism of osteoporoses and the bone mass effects of mechanical and nonmechanical agents. Bone Miner. 1987;2:73–85. [PubMed] [Google Scholar]
- 34.Frost HM. Bone’s mechanostat: a 2003 update. Anat Rec A Discov Mol Cell Evol Biol. 2003;275:1081–101. doi: 10.1002/ar.a.10119. [DOI] [PubMed] [Google Scholar]
- 35.Hart NH, Nimphius S, Weber J, et al. Musculoskeletal Asymmetry in Football Athletes: A Product of Limb Function over Time. Med Sci Sports Exerc. 2016;48:1379–87. doi: 10.1249/MSS.0000000000000897. [DOI] [PubMed] [Google Scholar]
- 36.Ergun M, Islegen C, Taskiran E. A cross-sectional analysis of sagittal knee laxity and isokinetic muscle strength in soccer players. Int J Sports Med. 2004;25:594–8. doi: 10.1055/s-2004-821116. [DOI] [PubMed] [Google Scholar]
- 37.Eniseler N, Sahan C, Vurgun H, Mavi HF. Isokinetic Strength Responses to Season-long Training and Competition in Turkish Elite Soccer Players. J Hum Kinet. 2012;31:159–68. doi: 10.2478/v10078-012-0017-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Cometti G, Maffiuletti NA, Pousson M, Chatard JC, Maffulli N. Isokinetic strength and anaerobic power of elite, subelite and amateur French soccer players. Int J Sports Med. 2001;22:45–51. doi: 10.1055/s-2001-11331. [DOI] [PubMed] [Google Scholar]
- 39.Brophy RH, Backus S, Kraszewski AP, et al. Differences between sexes in lower extremity alignment and muscle activation during soccer kick. J Bone Joint Surg Am. 2010;92:2050–8. doi: 10.2106/JBJS.I.01547. [DOI] [PubMed] [Google Scholar]
- 40.Brooks KA, Clark SL, Dawes JJ. Isokinetic Strength and Performance in Collegiate Women’s Soccer. J Nov Physiother. 2013;(Suppl 3):001. doi: 10.4172/2165-7025.S3-001. [DOI] [PubMed] [Google Scholar]
- 41.Coyle EF, Feiring DC, Rotkis TC, et al. Specificity of power improvements through slow and fast isokinetic training. J Appl Physiol Respir Environ Exerc Physiol. 1981;51:1437–42. doi: 10.1152/jappl.1981.51.6.1437. [DOI] [PubMed] [Google Scholar]