Apolipoprotein A-V is a protein that in humans is encoded by the APOA5 gene on chromosome 11.[5][6][7] It is significantly expressed in liver.[8] The protein encoded by this gene is an apolipoprotein and an important determinant of plasma triglyceride levels, a major risk factor for coronary artery disease. It is a component of several lipoprotein fractions including VLDL, HDL, chylomicrons. It is believed that apoA-V affects lipoprotein metabolism by interacting with LDL-R gene family receptors.[9] Considering its association with lipoprotein levels, APOA5 is implicated in metabolic syndrome.[10] The APOA5 gene also contains one of 27 SNPs associated with increased risk of coronary artery disease.[11]




Discovery
editThe gene for apolipoprotein A5 (APOA5, gene ID 116519, OMIM accession number – 606368) was originally found by comparative sequencing of human and mice DNA as a last member of the gene cluster of apolipoproteins APOA1/APOC3/APOA4/APOA5, located on human chromosome 11 at position 11q23.[5] The creation of two mice models (APOA5 transgenic and APOA5 knock-out) confirmed the important role of this gene in plasma triglyceride determination. The transgenic mice had lower and the knock-out mice higher levels of plasma triglycerides, while plasma cholesterol levels remained unchanged in both animal models. A Dutch group simultaneously described an identical gene as apolipoprotein which it is associated with the early phase of liver regeneration, but failed to recognise its important role in the determination of plasma triglyceride levels.[6]
Structure
editGene
editThe APOA5 gene resides on chromosome 11 at the band 11q23 and contains 4 exons and 3 introns.[7][12] This gene uses alternate polyadenylation sites and is located proximal to the apolipoprotein gene cluster on chromosome 11q23.[7]
Protein
editThis protein belongs to the apolipoprotein A1/A4/E family and contains 2 coiled coil domains.[7] Overall, APOA5 is predicted to have approximately 60% a-helical content.[6] The mature APOA5 protein spans a length of 366 amino acid residues, of which 23 amino acids code for the signal peptide.[13] The molecular mass of the precursor was calculated to be 41 kDa, while the mature APOA5 protein was calculated to be 39 kDa.[6]
Tissue distribution
editIn humans, APOA5 is expressed almost exclusively in the liver tissue;[5] some minor expressions have also been detected in the small intestine.[14] Nothing is known about the existence of the potential alternative splicing variants of this gene. In comparison with other apolipoproteins, plasma concentration of APOA5 is very low (less than 1 μg/mL).[15] This suggests that it has more catalytic than structural functions, since there is less than one APOA5 molecule per one lipoprotein particle. APOA5 is associated predominantly with TG-rich lipoproteins (chylomicrons and VLDL) and has also been detected on HDL particles.
Function
editAPOA5 mainly functions to influence plasma triglyceride levels.[16] The first suggested mechanism supposes that APOA5 functions as an activator of lipoprotein lipase (which is a key enzyme in triglyceride catabolism) and, through this process, enhances the metabolism of TG-rich particles. The second is the possible effect of APOA5 on the secretion of VLDL particles, since APOA5 reduces hepatic production by inhibiting VLDL-particle production and assembly by binding to cellular membranes and lipids.[17] Finally, the third possibility relates to the acceleration of the hepatic uptake of lipoprotein remnants and it has been shown that APOA5 binds to different members of the low-density lipoprotein receptor family.[18] In addition to its TG-lowering effect, APOA5 also plays a significant role in modulating HDL maturation and cholesterol metabolism. Increased APOA5 levels were associated with skewed cholesterol distribution from VLDL to large HDL particles.[19][20] APOA5 mRNA is upregulated during liver regeneration and this suggests that APOA5 serves a function in hepatocyte proliferation.[6] It’s also reported that APOA5 could enhance insulin secretion in beta-cells and the cell surface midkine could be involved in APOA5 endocytosis.[21]
Gene variability
editWithin the APOA5 gene, a couple of important SNPs with a widely confirmed effect on plasma TG levels as well as rare mutations have been described. In Caucasians, the common variants are inherited mostly in three haplotypes, which are characterised by two SNPs, namely rs662799 (T-1131>C; in almost complete LD with A-3>G, where the minor allele is associated with about 50% lower gene expression) and rs3135506 (Ser19>Trp; C56>G; alters the signal peptide and influences APOA5 secretion into plasma). There are also a further three common variants (A-3>G, IVS+476 G>A and T1259>C) which are not necessary for haplotype characterisation. Population frequencies of common APOA5 alleles exhibit large interethnic differences. For example, there are about 15% of carriers of the rs66299(C) allele among Caucasians, but the frequency could reach even between 40% and 50% among Asians. In contrast, the Trp19 allele is very rare in the Asian population (less than 1% of carriers) but is common in Caucasians (about 15% of carriers). Vice versa, important SNP (rs2075291, G553T, Gly185>Cys) with a population frequency of about 5% has been detected among Asians, but it is extremely rare among Caucasians. Sporadic publications refer to some other common polymorphisms, e.g. Val153>Met (rs3135507, G457A) and also suggest significant sex-dependent associations[22] with plasma lipids. Rare variants within the APOA5 gene have been described in a couple of different populations. Among the “common mutations/rare SNPs”, one of the most characterised on a population level is the Ala315>Val[23] exchange. Originally detected in patients with extreme TG levels over 10 mmol/L, it was also found in about 0.7% of the general population (mostly in individuals with normal TG values), which suggests a low penetrance of this variant. More than twenty other rare variants (mutations) have been described within the human APOA5 gene. They cover a wide spectrum that includes premature stop codons, amino acid changes as well as insertions and deletions. These mutations are generally associated with hypertriglyceridaemia, but penetration is usually not 100%. Individual mutations have been found mostly in one pedigree only.[24]
Not all the SNPs have a detrimental effect on TG levels. A recent report, showed that, in the Sardinian population, the missense mutation Arg282Ser in the APOA5 gene correlates with a decrease in TG levels. The authors believe that this point mutation is a major modulator of TG values in this population.[25]
Clinical significance
editIn humans, plasma triglycerides such as triacylglycerols have been long debated as an important risk factor for not only cardiovascular disease[26] but also for other relevant morbidities, such as cancer, renal disease, suicide, and all-cause mortality.[27] The APOA5 gene was found by comparative sequencing of ~200 kbp of human and mice DNA as the last member of the gene cluster of apolipoproteins located on human chromosome 11 at 11q23. Two mouse transgenic mouse models (APOA5 transgenic and APOA5 knockout) confirmed the important role of this gene in plasma triglyceride levels of plasma triglycerides. Obesity and metabolic syndrome are both closely related to plasma triglyceride levels and APOA5. Recent meta-analyses suggest that the effect on metabolic syndrome development is more profound for rs662799 in Asian population and for rs3135506 for Europeans.[10][28][29] Moreover, meta-analysis that focused on rs662799 and the risk of type 2 diabetes mellitus has suggested a significant association in Asian populations, but not in European populations.[30][31]
As a risk factor
editEven though plasma concentration of APOA5 is very low, some studies have focused on the analysis of the potential association of this biochemical parameter with cardiovascular disease (CVD). This relationship remains controversial, as higher plasma levels of APOA5 in individuals with CVD disease have been found in some, but not in all studies.[32][33]
Plasma lipids and cardiovascular disease
editThe major effect of the apolipoprotein A5 gene (and its variants) is on plasma triglyceride levels. Minor alleles (C1131 and Trp19) are primarily associated with the elevation of plasma triglyceride levels. The most extensive information available has been drawn from Caucasian populations, particularly in relation to the rs662799 SNP. Here, one minor allele is associated with an approximate 0.25 mmol/L increase of plasma TG levels.[34] A similar effect is associated with the Trp19 allele, even though it has not been confirmed by a large number of studies. Original studies have further described that the strongest effect of APOA5 polymorphisms on plasma TG levels is observed among Hispanics, with only minor effects detected among Africans. Among Asians, the effect on plasma TG levels is similar to that found among Caucasians. Generally, studies have suggested significant interethnic differences and in some cases sex-dependent associations as well.[22][35][36]
Sporadic publications have also mentioned a weak but nonetheless significant effect of APOA5 variants on plasma HDL-cholesterol and non-HDL cholesterol levels. [citation needed]
Myocardial infarction
editA large meta-analysis of 101 studies[34] confirmed a risk associated with the presence of the minor APOA5 allele -1131C and coronary heart disease. The odds ratio was 1.18 for every C allele. There are far fewer studies on the second common APOA5 polymorphism, Ser19>Trp, even though available studies have detected that its effect on plasma triglycerides is similar to C-1131>T. Nevertheless, the minor Trp allele is also associated with increased risk of CVD, and it seems that especially homozygotes and carriers of more minor alleles (both -1131C and 19Trp) are at higher risk of CVD.[37]
Clinical marker
editA multi-locus genetic risk score study based on a combination of 27 loci, including the APOA5 gene, identified individuals at increased risk for both incident and recurrent coronary artery disease events, as well as an enhanced clinical benefit from statin therapy. The study was based on a community cohort study (the Malmo Diet and Cancer study) and four additional randomized controlled trials of primary prevention cohorts (JUPITER and ASCOT) and secondary prevention cohorts (CARE and PROVE IT-TIMI 22).[11]
BMI, metabolic syndrome
editObesity and metabolic syndrome are both closely related to plasma triglyceride levels. Therefore, the focus on an association between APOA5 and BMI or metabolic syndrome is understandable. Available studies show that minor APOA5 alleles could be associated with an enhanced risk of obesity or metabolic syndrome development. However, genome wide studies have failed to prove that APOA5 is a gene associated with BMI values and/or obesity, so the effect could be far from clinically significant or at least significantly context-dependent.
Nutri-, acti- and pharmacogenetic associations
editSeveral studies have focused on changes of anthropometrical (body weight, BMI, WHR,…) or biochemical parameters (mostly plasma lipid levels) as a result of the interactions between common APOA5 variants and dietary habits (polyunsaturated fatty acid intake, n-3 and n-6 fatty acid intake, total fat and total energy intake, alcohol intake), dietary (lowering the energy intake) and/or physical activity interventions or dyslipidaemic (using statins or fenofibrate) treatment. Due to the high heterogeneity of the examined populations, differences in protocol and/or interventions used, the studies are difficult to directly compare and draw definitive conclusions.[38][39][40][41][42][43] However, with caution, it could be concluded that carriers of the minor C-1131, Trp19, or T553 alleles are in some cases less prone to the positive effects of environmental and/or pharmacological interventions. Some papers suggest the importance of the interactions between APOA5 and other genes, especially with common APOE (OMIM acc. No. 107741) three allelic (E2, E3, and E4) polymorphism, in the modulation of plasma lipids. In these cases, the interaction between minor alleles of both genes seems to be of importance. In the general population, APOE4 seems to have the potential to diminish the effect of minor APOA5 rs662799 and rs3135506 alleles, especially in females. Interaction between APOE and APOA5 Ser19˃Trp has been suggested to play some role in the development of type III hyperlipidaemia.[44] Further studies, in which interaction with APOA5 has been described, have included, for example, variants within FTO, lipoprotein lipase, USF-1 and FEN-1. They have also focused not only on plasma lipids, but on BMI values or hypertension as well.
Other roles
editSome other possible roles of APOA5 variants have been discussed, but generally these reports comprise only one or two papers – and first original papers with positive findings are usually not confirmed in second publications. These papers focus on the possible effect of different APOA5 variants on maternal height, longer foetal birth length, putative associations with plasma levels of C-reactive protein, LDL particle size and haemostatic markers. Despite the very low plasma concentration, variants within apolipoprotein A5 are potent determinants of plasma triglyceride levels. Minor alleles of three SNPs (rs662799, rs3135506, rs3135507) are associated with the higher risk of cardiovascular disease.
Interactive pathway map
editClick on genes, proteins and metabolites below to link to respective articles. [§ 1]
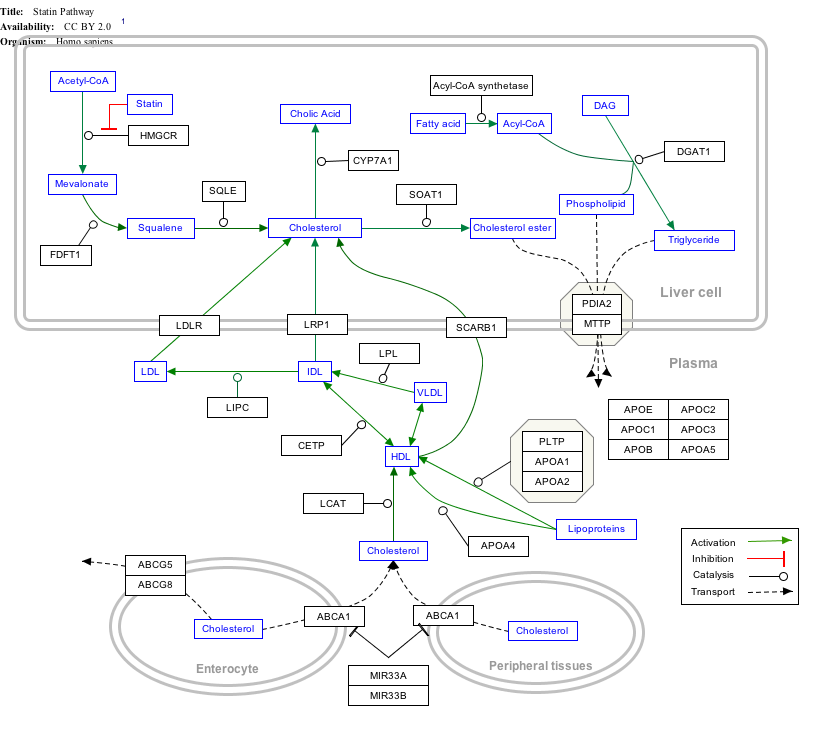
{kind=link}
- ^ The interactive pathway map can be edited at WikiPathways: "Statin_Pathway_WP430".
See also
editNotes
edit
The 2016 version of this article was updated by an external expert under a dual publication model. The corresponding academic peer reviewed article was published in Gene and can be cited as: Jaroslav A Hubacek (2 August 2016). "Apolipoprotein A5 fifteen years anniversary: Lessons from genetic epidemiology". Gene. Gene Wiki Review Series. 592 (1): 193–199. doi:10.1016/J.GENE.2016.07.070. ISSN 0378-1119. PMID 27496343. Wikidata Q28277677. |
References
edit- ^ a b c GRCh38: Ensembl release 89: ENSG00000110243 – Ensembl, May 2017
- ^ a b c GRCm38: Ensembl release 89: ENSMUSG00000032079 – Ensembl, May 2017
- ^ "Human PubMed Reference:". National Center for Biotechnology Information, U.S. National Library of Medicine.
- ^ "Mouse PubMed Reference:". National Center for Biotechnology Information, U.S. National Library of Medicine.
- ^ a b c Pennacchio LA, Olivier M, Hubacek JA, Cohen JC, Cox DR, Fruchart JC, Krauss RM, Rubin EM (October 2001). "An apolipoprotein influencing triglycerides in humans and mice revealed by comparative sequencing". Science. 294 (5540): 169–73. Bibcode:2001Sci...294..169P. doi:10.1126/science.1064852. OSTI 789171. PMID 11588264. S2CID 42251337.
- ^ a b c d e van der Vliet HN, Sammels MG, Leegwater AC, Levels JH, Reitsma PH, Boers W, Chamuleau RA (November 2001). "Apolipoprotein A-V: a novel apolipoprotein associated with an early phase of liver regeneration". The Journal of Biological Chemistry. 276 (48): 44512–20. doi:10.1074/jbc.M106888200. PMID 11577099.
- ^ a b c d "Entrez Gene: APOA5 apolipoprotein A-V".
- ^ "BioGPS - your Gene Portal System". biogps.org. Retrieved 2016-10-11.
- ^ Nilsson SK, Christensen S, Raarup MK, Ryan RO, Nielsen MS, Olivecrona G (September 2008). "Endocytosis of apolipoprotein A-V by members of the low density lipoprotein receptor and the VPS10p domain receptor families". The Journal of Biological Chemistry. 283 (38): 25920–7. doi:10.1074/jbc.M802721200. PMC 2533778. PMID 18603531.
- ^ a b Xu C, Bai R, Zhang D, Li Z, Zhu H, Lai M, Zhu Y (2013-01-01). "Effects of APOA5 -1131T>C (rs662799) on fasting plasma lipids and risk of metabolic syndrome: evidence from a case-control study in China and a meta-analysis". PLOS ONE. 8 (2): e56216. Bibcode:2013PLoSO...856216X. doi:10.1371/journal.pone.0056216. PMC 3585417. PMID 23468858.
- ^ a b Mega JL, Stitziel NO, Smith JG, Chasman DI, Caulfield MJ, Devlin JJ, Nordio F, Hyde CL, Cannon CP, Sacks FM, Poulter NR, Sever PS, Ridker PM, Braunwald E, Melander O, Kathiresan S, Sabatine MS (June 2015). "Genetic risk, coronary heart disease events, and the clinical benefit of statin therapy: an analysis of primary and secondary prevention trials". Lancet. 385 (9984): 2264–71. doi:10.1016/S0140-6736(14)61730-X. PMC 4608367. PMID 25748612.
- ^ Thierry-Mieg D, Thierry-Mieg J. "AceView: Gene:APOA5, a comprehensive annotation of human, mouse and worm genes with mRNAs or ESTsAceView". www.ncbi.nlm.nih.gov. Retrieved 2016-10-11.
- ^ Sharma V, Ryan RO, Forte TM (May 2012). "Apolipoprotein A-V dependent modulation of plasma triacylglycerol: a puzzlement". Biochimica et Biophysica Acta (BBA) - Molecular and Cell Biology of Lipids. 1821 (5): 795–9. doi:10.1016/j.bbalip.2011.12.002. PMC 3319174. PMID 22209939.
- ^ Guardiola M, Alvaro A, Vallvé JC, Rosales R, Solà R, Girona J, Serra N, Duran P, Esteve E, Masana L, Ribalta J (September 2012). "APOA5 gene expression in the human intestinal tissue and its response to in vitro exposure to fatty acid and fibrate". Nutrition, Metabolism, and Cardiovascular Diseases. 22 (9): 756–62. doi:10.1016/j.numecd.2010.12.003. PMID 21489765.
- ^ O'Brien PJ, Alborn WE, Sloan JH, Ulmer M, Boodhoo A, Knierman MD, Schultze AE, Konrad RJ (February 2005). "The novel apolipoprotein A5 is present in human serum, is associated with VLDL, HDL, and chylomicrons, and circulates at very low concentrations compared with other apolipoproteins". Clinical Chemistry. 51 (2): 351–9. doi:10.1373/clinchem.2004.040824. PMID 15528295.
- ^ Nilsson SK, Heeren J, Olivecrona G, Merkel M (November 2011). "Apolipoprotein A-V; a potent triglyceride reducer". Atherosclerosis. 219 (1): 15–21. doi:10.1016/j.atherosclerosis.2011.07.019. PMID 21831376.
- ^ Beckstead JA, Oda MN, Martin DD, Forte TM, Bielicki JK, Berger T, Luty R, Kay CM, Ryan RO (August 2003). "Structure-function studies of human apolipoprotein A-V: a regulator of plasma lipid homeostasis". Biochemistry. 42 (31): 9416–23. doi:10.1021/bi034509t. PMID 12899628.
- ^ Nilsson SK, Lookene A, Beckstead JA, Gliemann J, Ryan RO, Olivecrona G (March 2007). "Apolipoprotein A-V interaction with members of the low density lipoprotein receptor gene family". Biochemistry. 46 (12): 3896–904. doi:10.1021/bi7000533. PMID 17326667.
- ^ van der Vliet HN, Schaap FG, Levels JH, Ottenhoff R, Looije N, Wesseling JG, Groen AK, Chamuleau RA (August 2002). "Adenoviral overexpression of apolipoprotein A-V reduces serum levels of triglycerides and cholesterol in mice". Biochemical and Biophysical Research Communications. 295 (5): 1156–9. doi:10.1016/s0006-291x(02)00808-2. PMID 12135615.
- ^ Qu S, Perdomo G, Su D, D'Souza FM, Shachter NS, Dong HH (July 2007). "Effects of apoA-V on HDL and VLDL metabolism in APOC3 transgenic mice". Journal of Lipid Research. 48 (7): 1476–87. doi:10.1194/jlr.M600498-JLR200. PMC 2665252. PMID 17438339.
- ^ Helleboid-Chapman A, Nowak M, Helleboid S, Moitrot E, Rommens C, Dehondt H, Héliot L, Drobecq H, Fruchart-Najib J, Fruchart JC (2009-01-01). "Apolipoprotein A-V modulates insulin secretion in pancreatic beta-cells through its interaction with midkine". Cellular Physiology and Biochemistry. 24 (5–6): 451–60. doi:10.1159/000257484. PMID 19910685.
- ^ a b Hubacek JA, Skodová Z, Adámková V, Lánská V, Poledne R (December 2005). "Sex-specific effect of APOAV variant (Val153>Met) on plasma levels of high-density lipoprotein cholesterol". Metabolism. 54 (12): 1632–5. doi:10.1016/j.metabol.2005.06.012. PMID 16311097.
- ^ Hubacek JA, Wang WW, Skodová Z, Adámková V, Vráblík M, Horínek A, Stulc T, Ceska R, Talmud PJ (2008). "APOA5 Ala315>Val, identified in patients with severe hypertriglyceridemia, is a common mutation with no major effects on plasma lipid levels". Clinical Chemistry and Laboratory Medicine. 46 (6): 773–7. doi:10.1515/CCLM.2008.160. PMID 18601597. S2CID 11445384.
- ^ Melegh BI, Duga B, Sümegi K, Kisfali P, Maász A, Komlósi K, Hadzsiev K, Komoly S, Kosztolányi G, Melegh B (2012). "Mutations of the apolipoprotein A5 gene with inherited hypertriglyceridaemia: review of the current literature". Current Medicinal Chemistry. 19 (36): 6163–70. doi:10.2174/092986712804485719 (inactive 1 November 2024). PMID 23150946.
{{cite journal}}: CS1 maint: DOI inactive as of November 2024 (link) - ^ Sidore C, Busonero F, Maschio A, Porcu E, Naitza S, Zoledziewska M, et al. (November 2015). "Genome sequencing elucidates Sardinian genetic architecture and augments association analyses for lipid and blood inflammatory markers". Nature Genetics. 47 (11): 1272–81. doi:10.1038/ng.3368. PMC 4627508. PMID 26366554.
- ^ Miller M, Stone NJ, Ballantyne C, Bittner V, Criqui MH, Ginsberg HN, Goldberg AC, Howard WJ, Jacobson MS, Kris-Etherton PM, Lennie TA, Levi M, Mazzone T, Pennathur S (May 2011). "Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association". Circulation. 123 (20): 2292–333. doi:10.1161/CIR.0b013e3182160726. PMID 21502576.
- ^ Hubacek JA (October 2016). "Apolipoprotein A5 fifteen years anniversary: Lessons from genetic epidemiology". Gene. 592 (1): 193–9. doi:10.1016/j.gene.2016.07.070. PMC 7108956. PMID 27496343.
- ^ Liu CF, Yang QF, Chen XL, Liu CY (October 2012). "Apolipoprotein a5 gene polymorphism and risk for metabolic syndrome: a meta-analysis". Genetic Testing and Molecular Biomarkers. 16 (10): 1241–5. doi:10.1089/gtmb.2012.0183. PMID 22905904.
- ^ Jiang CQ, Liu B, Cheung BM, Lam TH, Lin JM, Li Jin Y, Yue XJ, Ong KL, Tam S, Wong KS, Tomlinson B, Lam KS, Thomas GN (November 2010). "A single nucleotide polymorphism in APOA5 determines triglyceride levels in Hong Kong and Guangzhou Chinese". European Journal of Human Genetics. 18 (11): 1255–60. doi:10.1038/ejhg.2010.93. PMC 2987477. PMID 20571505.
- ^ Lee KH, Kim OY, Lim HH, Lee YJ, Jang Y, Lee JH (November 2010). "Contribution of APOA5-1131C allele to the increased susceptibility of diabetes mellitus in association with higher triglyceride in Korean women". Metabolism. 59 (11): 1583–90. doi:10.1016/j.metabol.2010.02.008. PMID 20303129.
- ^ Yin YW, Sun QQ, Wang PJ, Qiao L, Hu AM, Liu HL, Wang Q, Hou ZZ (2014-01-01). "Genetic polymorphism of apolipoprotein A5 gene and susceptibility to type 2 diabetes mellitus: a meta-analysis of 15,137 subjects". PLOS ONE. 9 (2): e89167. Bibcode:2014PLoSO...989167Y. doi:10.1371/journal.pone.0089167. PMC 3929635. PMID 24586566.
- ^ Yang Y, Walijee SM, Jin J, Zhao SP, Peng DQ (2012). "Serum apolipoprotein A-V in patients with coronary artery disease and its association with triglyceride". Journal of Clinical Lipidology. 6 (5): 462–8. doi:10.1016/j.jacl.2012.02.004. PMID 23009782.
- ^ Manpuya MW, Guo J, Zhao Y (March 2001). "The relationship between plasma apolipoprotein A-IV levels and coronary heart disease". Chinese Medical Journal. 114 (3): 275–9. PMID 11780313.
- ^ a b Sarwar N, Sandhu MS, Ricketts SL, Butterworth AS, Di Angelantonio E, Boekholdt SM, Ouwehand W, Watkins H, Samani NJ, Saleheen D, Lawlor D, Reilly MP, Hingorani AD, Talmud PJ, Danesh J (May 2010). "Triglyceride-mediated pathways and coronary disease: collaborative analysis of 101 studies". Lancet. 375 (9726): 1634–9. doi:10.1016/S0140-6736(10)60545-4. PMC 2867029. PMID 20452521.
- ^ Pennacchio LA, Olivier M, Hubacek JA, Krauss RM, Rubin EM, Cohen JC (November 2002). "Two independent apolipoprotein A5 haplotypes influence human plasma triglyceride levels". Human Molecular Genetics. 11 (24): 3031–8. doi:10.1093/hmg/11.24.3031. PMID 12417524.
- ^ Lai CQ, Tai ES, Tan CE, Cutter J, Chew SK, Zhu YP, Adiconis X, Ordovas JM (December 2003). "The APOA5 locus is a strong determinant of plasma triglyceride concentrations across ethnic groups in Singapore". Journal of Lipid Research. 44 (12): 2365–73. doi:10.1194/jlr.M300251-JLR200. PMID 12951359.
- ^ Hubacek JA, Skodová Z, Adámková V, Lánská V, Poledne R (February 2004). "The influence of APOAV polymorphisms (T-1131>C and S19>W) on plasma triglyceride levels and risk of myocardial infarction". Clinical Genetics. 65 (2): 126–30. doi:10.1111/j.0009-9163.2004.00199.x. PMID 14984471. S2CID 34501809.
- ^ Lai CQ, Corella D, Demissie S, Cupples LA, Adiconis X, Zhu Y, Parnell LD, Tucker KL, Ordovas JM (May 2006). "Dietary intake of n-6 fatty acids modulates effect of apolipoprotein A5 gene on plasma fasting triglycerides, remnant lipoprotein concentrations, and lipoprotein particle size: the Framingham Heart Study". Circulation. 113 (17): 2062–70. doi:10.1161/CIRCULATIONAHA.105.577296. hdl:10550/18832. PMID 16636175.
- ^ Liu Y, Ordovas JM, Gao G, Province M, Straka RJ, Tsai MY, Lai CQ, Zhang K, Borecki I, Hixson JE, Allison DB, Arnett DK (February 2009). "Pharmacogenetic association of the APOA1/C3/A4/A5 gene cluster and lipid responses to fenofibrate: the genetics of lipid-lowering drugs and diet network study". Pharmacogenetics and Genomics. 19 (2): 161–9. doi:10.1097/FPC.0b013e32831e030e. PMC 2733171. PMID 19057464.
- ^ Hubacek JA, Adamkova V, Prusikova M, Snejdrlova M, Hirschfeldova K, Lanska V, Ceska R, Vrablik M (June 2009). "Impact of apolipoprotein A5 variants on statin treatment efficacy". Pharmacogenomics. 10 (6): 945–50. doi:10.2217/pgs.09.17. PMID 19530961.
- ^ Sánchez-Moreno C, Ordovás JM, Smith CE, Baraza JC, Lee YC, Garaulet M (March 2011). "APOA5 gene variation interacts with dietary fat intake to modulate obesity and circulating triglycerides in a Mediterranean population". The Journal of Nutrition. 141 (3): 380–5. doi:10.3945/jn.110.130344. PMC 3040902. PMID 21209257.
- ^ Hishida A, Morita E, Naito M, Okada R, Wakai K, Matsuo K, Nakamura K, Takashima N, Suzuki S, Takezaki T, Mikami H, Ohnaka K, Watanabe Y, Uemura H, Kubo M, Tanaka H, Hamajima N (2012). "Associations of apolipoprotein A5 (APOA5), glucokinase (GCK) and glucokinase regulatory protein (GCKR) polymorphisms and lifestyle factors with the risk of dyslipidemia and dysglycemia in Japanese - a cross-sectional data from the J-MICC Study". Endocrine Journal. 59 (7): 589–99. doi:10.1507/endocrj.ej11-0310. PMID 22517333.
- ^ Hubacek JA, Peasey A, Kubinova R, Pikhart H, Bobak M (March 2014). "The association between APOA5 haplotypes and plasma lipids is not modified by energy or fat intake: the Czech HAPIEE study". Nutrition, Metabolism, and Cardiovascular Diseases. 24 (3): 243–7. doi:10.1016/j.numecd.2013.08.008. PMC 4357849. PMID 24462044.
- ^ Schaefer JR, Sattler AM, Hackler B, Kurt B, Hackler R, Maisch B, Soufi M (November 2004). "Hyperlipidemia in patients with apolipoprotein E 2/2 phenotype: apolipoprotein A5 S19W mutation as a cofactor". Clinical Chemistry. 50 (11): 2214. doi:10.1373/clinchem.2004.037689. PMID 15502102.
External links
edit- Human APOA5 genome location and APOA5 gene details page in the UCSC Genome Browser.
Further reading
edit- Garelnabi M, Lor K, Jin J, Chai F, Santanam N (January 2013). "The paradox of ApoA5 modulation of triglycerides: evidence from clinical and basic research". Clinical Biochemistry. 46 (1–2): 12–9. doi:10.1016/j.clinbiochem.2012.09.007. PMC 3534811. PMID 23000317.
- Hubacek JA (2005). "Apolipoprotein A5 and triglyceridemia. Focus on the effects of the common variants". Clinical Chemistry and Laboratory Medicine. 43 (9): 897–902. doi:10.1515/CCLM.2005.153. PMID 16176166. S2CID 20630818.
- Hubácek JA, Adámková V, Vrablík M, Kadlecová M, Zicha J, Kunes J, Pitha J, Suchánek P, Poledne R (2009). "Apolipoprotein A5 in health and disease". Physiological Research. 58 (Suppl 2): S101–9. doi:10.33549/physiolres.931911. PMID 20131928.
- Sharma V, Forte TM, Ryan RO (April 2013). "Influence of apolipoprotein A-V on the metabolic fate of triacylglycerol". Current Opinion in Lipidology. 24 (2): 153–9. doi:10.1097/MOL.0b013e32835c8c1a. PMC 3645348. PMID 23241513.
- Tai ES, Ordovas JM (August 2008). "Clinical significance of apolipoprotein A5". Current Opinion in Lipidology. 19 (4): 349–54. doi:10.1097/MOL.0b013e328304b681. PMC 4428951. PMID 18607181.
- Pennacchio LA, Rubin EM (April 2003). "Apolipoprotein A5, a newly identified gene that affects plasma triglyceride levels in humans and mice". Arteriosclerosis, Thrombosis, and Vascular Biology. 23 (4): 529–34. doi:10.1161/01.ATV.0000054194.78240.45. PMID 12615678.
- Jakel H, Nowak M, Helleboid-Chapman A, Fruchart-Najib J, Fruchart JC (2006). "Is apolipoprotein A5 a novel regulator of triglyceride-rich lipoproteins?". Annals of Medicine. 38 (1): 2–10. doi:10.1080/07853890500407488. PMID 16448983. S2CID 39125761.
- Calandra S, Priore Oliva C, Tarugi P, Bertolini S (April 2006). "APOA5 and triglyceride metabolism, lesson from human APOA5 deficiency". Current Opinion in Lipidology. 17 (2): 122–7. doi:10.1097/01.mol.0000217892.00618.54. PMID 16531747.
- Wong K, Ryan RO (June 2007). "Characterization of apolipoprotein A-V structure and mode of plasma triacylglycerol regulation". Current Opinion in Lipidology. 18 (3): 319–24. doi:10.1097/MOL.0b013e328133856c. PMID 17495607. S2CID 5553393.
- Nabika T, Nasreen S, Kobayashi S, Masuda J (December 2002). "The genetic effect of the apoprotein AV gene on the serum triglyceride level in Japanese". Atherosclerosis. 165 (2): 201–4. doi:10.1016/S0021-9150(02)00252-6. PMID 12417270.
- Pennacchio LA, Olivier M, Hubacek JA, Krauss RM, Rubin EM, Cohen JC (November 2002). "Two independent apolipoprotein A5 haplotypes influence human plasma triglyceride levels". Human Molecular Genetics. 11 (24): 3031–8. doi:10.1093/hmg/11.24.3031. PMID 12417524.
- Talmud PJ, Hawe E, Martin S, Olivier M, Miller GJ, Rubin EM, Pennacchio LA, Humphries SE (November 2002). "Relative contribution of variation within the APOC3/A4/A5 gene cluster in determining plasma triglycerides". Human Molecular Genetics. 11 (24): 3039–46. doi:10.1093/hmg/11.24.3039. PMID 12417525.
- Vu-Dac N, Gervois P, Jakel H, Nowak M, Bauge E, Dehondt H, Staels B, Pennacchio LA, Rubin EM, Fruchart-Najib J, Fruchart JC (May 2003). "Apolipoprotein A5, a crucial determinant of plasma triglyceride levels, is highly responsive to peroxisome proliferator-activated receptor alpha activators". The Journal of Biological Chemistry. 278 (20): 17982–5. doi:10.1074/jbc.M212191200. PMID 12637506.
- Prieur X, Coste H, Rodriguez JC (July 2003). "The human apolipoprotein AV gene is regulated by peroxisome proliferator-activated receptor-alpha and contains a novel farnesoid X-activated receptor response element". The Journal of Biological Chemistry. 278 (28): 25468–80. doi:10.1074/jbc.M301302200. hdl:2445/105706. PMID 12709436.
- Weinberg RB, Cook VR, Beckstead JA, Martin DD, Gallagher JW, Shelness GS, Ryan RO (September 2003). "Structure and interfacial properties of human apolipoprotein A-V". The Journal of Biological Chemistry. 278 (36): 34438–44. doi:10.1074/jbc.M303784200. PMID 12810715.
- Horínek A, Vráblík M, Ceska R, Adámková V, Poledne R, Hubacek JA (April 2003). "T-1131-->C polymorphism within the apolipoprotein AV gene in hypertriglyceridemic individuals". Atherosclerosis. 167 (2): 369–70. doi:10.1016/S0021-9150(03)00022-4. PMID 12818421.
- Kao JT, Wen HC, Chien KL, Hsu HC, Lin SW (October 2003). "A novel genetic variant in the apolipoprotein A5 gene is associated with hypertriglyceridemia". Human Molecular Genetics. 12 (19): 2533–9. doi:10.1093/hmg/ddg255. PMID 12915450.
- Vrablík M, Horínek A, Ceska R, Adámková V, Poledne R, Hubacek JA (August 2003). "Ser19-->Trp polymorphism within the apolipoprotein AV gene in hypertriglyceridaemic people". Journal of Medical Genetics. 40 (8): 105e–105. doi:10.1136/jmg.40.8.e105. PMC 1735562. PMID 12920097.
- Clark HF, Gurney AL, Abaya E, Baker K, Baldwin D, Brush J, Chen J, Chow B, Chui C, Crowley C, Currell B, Deuel B, Dowd P, Eaton D, Foster J, Grimaldi C, Gu Q, Hass PE, Heldens S, Huang A, Kim HS, Klimowski L, Jin Y, Johnson S, Lee J, Lewis L, Liao D, Mark M, Robbie E, Sanchez C, Schoenfeld J, Seshagiri S, Simmons L, Singh J, Smith V, Stinson J, Vagts A, Vandlen R, Watanabe C, Wieand D, Woods K, Xie MH, Yansura D, Yi S, Yu G, Yuan J, Zhang M, Zhang Z, Goddard A, Wood WI, Godowski P, Gray A (October 2003). "The secreted protein discovery initiative (SPDI), a large-scale effort to identify novel human secreted and transmembrane proteins: a bioinformatics assessment". Genome Research. 13 (10): 2265–70. doi:10.1101/gr.1293003. PMC 403697. PMID 12975309.